

Do Masks Work? They Are a Talisman.
Do Masks Work? They Are a Talisman.
Part 2: What Must be Done.

On 25 March 2022, Hawaii Governor David Ige bravely ended his State’s universal mask mandate. Leading by example, he ensured his state’s citizenry were the last beacons of healthy living to succumb to the overwhelming misinformation that they might survive without a DIY face covering. In a rare show of bipartisan support, Republican State Senator Kurt Fevella gave credit to the governor for not lifting the mandate sooner. Governor Ige let the clock run out and it wasn’t a moment to soon…
Don’t fret. Convinced the COVID-19 booster had made a temporary dent in the case count and hospitalization rate, he was ready to exercise his emergency authorities and reinstate the mandate whenever necessary.
It’s taken the entire community to get to this point, but we’ve seen variants knock out progress. If we see another surge, we will be ready to reinstate the mask policy, if needed.
Like several other States that had begun to scale back their mandates during the preceding weeks, he still required them in public schools, prisons, airports, and other similar indoor settings. Oregon and Washington made the risky decision to end theirs a few days prior, but fortunately for them, there were no serious health outcomes for those put at risk by their ‘reckless’ choices.
… Aside from Oregon Health Sciences University (OHSU) losing over a billion dollars between 2021 and 2022 in revenue as a result of excluding ongoing care for some of their more lucrative specialties. Thankfully they still had Ivy League educated professionals talking about the things that matter, masks.
COVID was that important. Cancer patients had to wait.
I always knew OHSU physician Esther Choo MD to be talented, smart, and a sincerely good person. She is brilliant. I know this to be a fact because we grew up together. We attended the same small school and lived in the same small town with the same circle of friends, but I can’t quite wrap my head around her opinion on masks. Part three of this Substack will cover the science surrounding mask efficacy, but she has been a vocal mask supporter on CNN, MSNBC, and social media, and her opinions aren’t really focused on the science. She had this to say about masking and educational outcomes.

This is a case of mental jiujitsu. The young were at almost no risk from COVID. Health bureaucrats established mitigation protocols completely delinked from actual science resulting in deleterious outcomes for the least advantaged in our country. Masks led to reduced language and social development, while many were pushed out of school regardless. Doctors support a solution for the problem health bureaucrats created, and it results in stunted development… and we are supposed to stand up and cheer!?!?
When I challenged Esther, a fierce advocate for minority rights, on the topics of masking on social media, I presented data. If you have read part one of this Substack series, you’ll know why I failed to convince her.
She decided to unfriend me. I suppose I am exhausting, but we all must wisely choose with whom we associate.
While Doctors were Dancing their way through a pandemic, we have been compiling data to help you resist future infringements of your liberty. One must first closely examine the details surrounding how the mandate was issued, but before going into the specific steps needed to resist another illegal executive overreach, let’s discuss the strategy of attack.
‘1000 Grains of Sand’ (一千沙砾) and Bureaucratic Guerrilla warfare
The Chinese have an intelligence collection methodology termed 1000 grains of sand. They collect seemingly innocuous data from thousands of sources. Each datapoint alone appears to be of limited value; however, when one brings it all together, the sheer volume of information provides an intelligence advantage.
When combatting new mandates, we must ask as many questions from as many sources as possible. We may feel we already know the answer, but it is very important that those who wish to impose future mandates are forced … dare I say coerced … into formally answering those questions.
Why?
We may be missing fundamental information that could help us thwart an illegal mandate. Perhaps yours is the grain of sand that completes our beach.
If one works in State or Federal government, it leaves a paper trail that could be the subject of Freedom of Information Act (FOIA) requests. It may also be useful in future litigation during the discovery process.
All questions force those attempting to implement a mandate to delay their plans. They must take time out of their day to answer. The more detailed the questions, the more time consuming the process. When we redirect resources towards untangling the specifics of a future mandate, it makes it the kind of difficult endeavor most choose to avoid.
This strategy is a double-edged sword. We must weigh one’s duty to keep the wheels of government moving against the cost associated with bureaucratic guerrilla warfare. In this case, deleterious policy decisions were far more damaging to workplace efficiency than the isolated but successful resistance to immoral orders.
The first step in fighting back is understanding the legal foundations.
The difference between a mandate and a law?
The first step one must take if they wish to resist illegal mandates is to determine exactly how and through what delegated agencies or representative bodies the mandate has been issued.
Mandates are enacted by either the Federal or State executive branch. They are temporary, usually put in place during a formally declared state of emergency, and quicker than enacting a law. In most cases, the mandate is issued as guidance through a subordinate agency. If the executive office delegates issuance of the mandate through a subordinate agency which is also authorized to act against those who disobey, it is enforceable. If it is a mandate that has not been delegated to a subordinate agency with enforcement authority, it is harder to legally enforce.
A law is a lengthier legislative process requiring input from all the appropriate elected representatives. It is enforceable under penalty of law.
In general, the authority for mask mandates is derived from three primary sources:
Local and State regulations that adhere to the Center for Disease Control and Prevention recommendations;
Executive orders for federal government employees;
The perception of a legal requirement.
Never presuppose the people you are dealing with have a full grasp of what they are enforcing. As we are all too aware, there is an army of functionaries willing to do as they’re told with little thought to the moral and legal implications. Always start with a cordial email including fundamental questions.
Please note, the email text provided is primarily intended for federal or state government employees, but it can be reworked to fit the needs of a privately employed individual. Included below is an example you should liberally plagiarize for your personal needs.
Good day,
I received notification that mask mandates are being reintroduced to the workplace. Can you provide additional details or forward my queries to the appropriate individual for response? Please see below questions.
Are we in a state of emergency allowing for a mandate of this nature? Please provide the date and link to the documentation related to the state of emergency.
Please provide the date and language for issuance of the mandate and a link where it has been formally published for public review.
When did the state of emergency begin and did the language of said mandate provide an end date or criteria to end the mandate? If not, what criteria do you, my employer, plan to include to ensure the workforce is burdened no more than necessary?
If criteria to end the mandate was included, either in the language of the mandate or through authority delegated to an agency or department, please provide that language. This also includes documenting the specific statutory authority delegated to said agency to end the mandate or the specific legal authority for the responsible executive to end the mandate.
Which agency or department issued the mandate or had delegated authority from the executive to issue the mandate? Please confirm whether the mask mandate was a recommendation or requirement.
If the agency issuing the mandate defined it as a requirement, please cite their specific enforcement authorities. What authorities to enforce a mandate have been provided by legislative action? Where has it been defined in the Administrative Procedure Act (APA)?
If that agency does not have enforcement authority, please provide details related to how the mandate will be enforced? If my employer intends to enforce the mandate, under what delegated authorities has enforcement been defined?
Has my employer published formal policy supporting enforcement of the mandate? If so, did my employer properly coordinate the policy and was there an opportunity for employee comment? Were committees and appropriate offices within my organization given the opportunity to coordinate? As you are aware, employee comment and coordination has been an effective means to avoid future legal and implementation disputes.
Can you provide documentation showing that my organization complied with all the regulatory and statutory requirements of the APA when establishing this policy? For example, if multiple agencies and departments were affected by the mandate, was there coordination between the agencies and departments to ensure that the implementation was consistent between all affected parties?
Did you coordinate all the above issues with my union? If so, what were their comments and questions? Were those questions answered? Did they also address the specifics of enforcement and disciplinary action, and request that you provide the regulatory and statutory requirements for both?
What is the proposed disciplinary action for those who do not comply with the mandate?
If formal published policy does not exist, what regulatory and or statutory authority authorizes disciplinary action against employees who do not comply? Please provide documentation showing that my employer can take disciplinary action without formally published policy.
With respect,
Employee Title and Name
Contact Information
Establishing that your employer understands the legal underpinnings of the mandate is just the first step in this process. Remember, if they chose to make the process onerous for you, then you should also ensure there is a steady, daily stream of detailed questions they must answer in writing if they seek to justify another unjustifiable mandate.
Maybe you could show us the data…
If you are in the United States and working for the federal government or any employer using Centers for Disease Control and Prevention (CDC) standards to justify mask mandates, then I suggest you ask that they provide proof that CDC’s data no longer requires regular readjustments as we have seen across many states in the US. This includes data identifying the age stratified risk profile, as working age adults are far less likely to endure serious outcomes. Data should also include the risk profile for vaccinated and unvaccinated individuals.
Good day,
I understand that our organization is instituting mask mandates. Before I decide whether I will undertake an experimental medical procedure, I would like you to provide additional information related to the data supporting this decision.
As you know, between 2020 and 2022 there were numerous mask mandates across the country. The CDC used case rates and hospitalizations to justify these highly coercive methods. Unfortunately, we repeatedly saw the data having to be revised downward after mandates had already exacted a heavy toll on average Americans.
Have you asked the CDC to provide additional information on their collection of data, and does it demonstrate the CDC has adopted a different model that would alleviate the faulty protocols previous employed? If you haven’t asked for this data, why and who specifically is responsible for this policy?
As you know, this mandate is being justified as a means to increase workforce efficiency. You have a requirement to ensure that the policy you have been delegated to implement addresses this need. I encourage you to read the following reports showing significant changes in case counts and death.
The Hill: Is Us COVID-19 Death Count Inflated?
Dr. Scott Jensen talks about inflation of COVID death.
Washington COVID death count inflated.
Experts confirm COVID deaths inflated.
As you are probably aware, there was a recent CDC report showing that the vaccinated were at higher risk for catching and transmitting coronavirus. With that in mind, would it not be appropriate to only ask those that have been vaccinated to test and mask? What does the data say in terms of risk differential between the vaccinated and unvaccinated?
Will we be seeking policies to distance the vaccinated from other vaccinated? Or perhaps, you are considering the nursing home method of containment employed in New York? Should we keep the vaccinated collocated to ensure those less likely to contract COVID and impact workforce efficiency remain healthy?
I am not advocating any of those policies; however, the unvaccinated were previously assessed to be at greater risk, requiring additional safety protocols. It seems like a natural extension of the policies previously employed.
Have you acquired data showing the risk profile for those previous infected? This should also include those previous infected by vaccination status.
We are lucky to have been gathering data in our workplace between 2020-2022. What does the data specific to our workforce show regarding mask efficacy? As our organization’s leadership team is ultimately responsible for workforce efficiency, I would hope that our internal data has been examined and we have definitively concluded that the desired effect will be achieved with this policy. Please share that data with the workforce.
Has all this data and any new data been shared with my union? Has my union responded?
With respect,
Employee Title and Name
Contact Information
Data is important, but not when contractors buying up Chinese made weapons of environmental destruction need a purchaser. If you have engaged this long, they have probably started to file your memos in the “crazies” bin, but don’t let that deter you.
Fraud, waste, and abuse is the business model.
Every organization has an established means of contracting for goods and services. The federal government’s contracting processes are defined in the Federal Acquisitions Regulation System (FARS) and each agency and department have their own regulations that further define the process. They are specific and have many stipulations to ensure that the opportunities for Fraud, Waste, and Abuse (FWA) are minimized to the extent possible. It is part of the reason the USG and DOD chose to use a highly unusual method of contracting services and goods for Operation Warp Speed (OWS). There was far less scrutiny.
You don’t need to know every regulation and law. All you need to know to fight illegal mandates is that contracts must define what they are purchasing from what company, for how much, and how long the contract exists. The USG is required to define explicitly what the product will do in the contract.
If the product is being purchased to prevent the spread of coronavirus in the workplace, it will state as such in the contract. Your next inquiries should focus on the specifics of the contract.
Good day,
As part of the masking mandate, my employer has provided masks in the workplace. I am concerned that this contractual agreement between the mask supplier and my organization may constitute Fraud, Waste, and Abuse (FWA). Perhaps you can help alleviate my concern.
Please provide a copy of the contract defining the terms of the agreement. If not, please explain why and under what authority you can refuse to provide the contractual agreement? Please also answer the following questions.
What company holds this contract and how did it acquire said contract? Were there competitive bids? Is it a US company or a foreign company? Is it US product or foreign made product? Does this company hold other contracts with our organization and for what products or services?
Does the contract explicitly define the proposed use of the mask? If so, can you provide the language in the contract?
How long does the contract last? Will this supplier continue to provide PPE pending future needs? Please define the timeframe of the contract.
Where will these masks be distributed? Is that defined in the contractual agreement, or is that entirely dependent on the organization? For example, are the masks going to be distributed in health care settings or for the public, or in every office. I ask this question, because most masking studies indicate they have been tested in health care settings vice for widespread use.
How much product will be ordered or has already been ordered? How did my organization conclude that this would meet workforce needs?
How much did the product cost? Please define per unit, and total cost to our organization.
Did we have any previous contracts for items similar or the same in terms of purpose? For example, were their other mask contracts between 2020-2023 that have since expired? Why are we no longer using those products? Can you provide the contract? If not, why and under what authority you can refuse to provide the contractual agreement?
With respect,
Employee Title and Name
Contact Information
Once the contractual details are defined, it makes it easier to dive into the specifics of the product.
Is it a Mask or a Respirator?
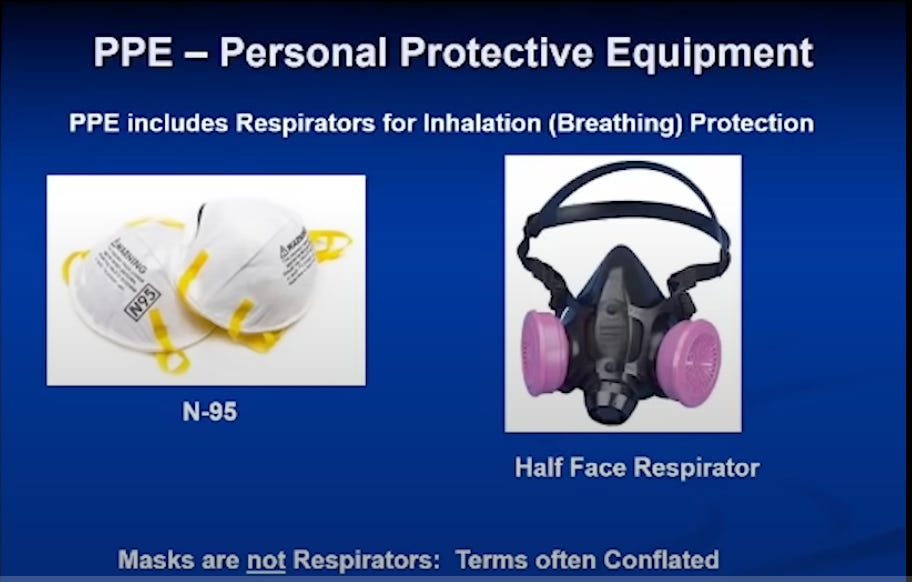
Masks are not respirators. Occupational Safety and Health Administration (OSHA) made that determination with respiratory protection standard (RPS) 29 CFR 134 1910.34. The only product capable of filtering for particles the size of a virus is a respirator. Surgical masks are not respirators, and cloth face coverings are not substitutes for respirators. They cannot be fit tested.
Below data is taken from the Petty Podcast. It clearly defines the differences between masks and respirators.
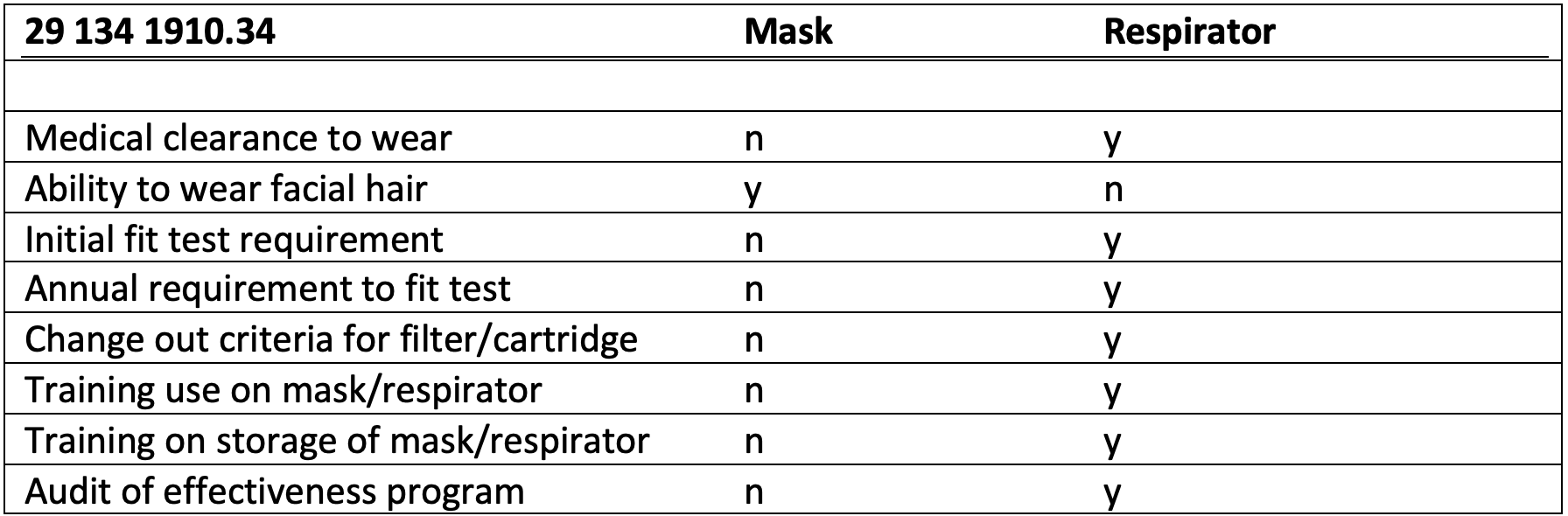
Respirators require a medical clearance because respiratory ailments like asthma limit long-term use. Now that we know the difference between masks and respirators, we can check and see if your employer knows how to differentiate.
Good day!
I respectfully request information about the masks being distributed to the workforce, and the types of masks approved for use to stop the spread of COVID.
Are these masks rated to stop the spread of a respiratory virus? Does the packaging material state it will stop the spread of a respiratory virus? Are there inserts or any other documentation included in the packaging that would indicate these masks or the masks we have been permitted to use at the office will be effective?
As you may be aware, OSHA respiratory protection standard (RPS) 29 CFR 134 1910.34 requires a medical clearance for use of a respirator. There are several other requirements that include: removal of facial hair, an initial test fit, annual requirement to test fit, frequent filter changes, training on use and storage of the respirator, and audits on program effectiveness. Under what authority is my employer circumventing these requirements and permitting the use of masks instead of respirators?
Assuming my employer has authority to ignore RPS 29 CFR 134 1910.34, I have several other questions.
Please advise where my employer has published those regulations for the employees to read. Did employees have an opportunity to comment on the change to OSHA regulations? Was this policy coordinated with OSHA or any other government agency, and if so, with which agency or department?
Was my union made aware of these workplace safety changes? If so, how did they rerspond?
Is a medical clearance required to wear a mask? The masks are being used in place of a respirator. Therefore, it seems reasonable our employer would apply the same high standards required by OSHA. If not, I urge you to look closely at recent studies showing the deleterious effects caused by CO2 build-up, toxic dyes, fomites, and bacterial growth on masks.
Is there a fit testing requirement? If so, are you providing training on proper fitting? Proper fitting may require removal of facial hair. Do you intend to provide updated personal grooming standards for the workforce? If so, has it been published? If it has not yet been published, will you provide an opportunity for employee comment?
What sort of training are you providing to ensure proper use, fitting, and replacement frequency? If there is no training being offered, why and how will you ensure this mitigation method will be effective?
Is there an industrial hygienist responsible for this program? If so, who is that person and are they available to field employee questions?
With respect,
Employee Title and Name
Contact Information
What is an industrial hygienist?

What is an industrial hygienist (IH)? They aren’t dentists. They are experts in workplace safety and are responsible for executing industrial measures that protect the workforce. They identify exposures that could cause workplace illness or injury and apply layered measures to promote safety. IH are primarily responsible for identifying and processing the following categories of the workplace hazards:
Chemical hazards like fumes and vapors.
Biological hazards like bacteria and viruses.
Physical hazards such as heat and radiation.
Ergonomic hazards such as lifting or pushing heavy machinery.
Air contaminants such as particles and aerosols.
Our employers have failed to recognize that COVID-19 is an aerosol and that requires engineering controls. Engineering controls focus on dilution and destruction of the aerosol contaminant; these are the most effective measures that can be taken to deal with COVID particles that are about .1 micron (µ) in size. Masking and personal protective gear are the least effective mitigation method.
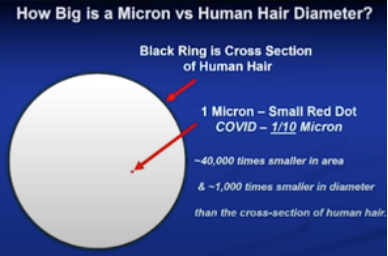
Aerosol plumes on release can move 7-8 meters, and its movement is governed by Brownian motion. Brownian motion is random. In comparison to droplets, aerosol plumes contain far more viral material, and they can stay suspended in the atmosphere for as long as 30 hours in a confined environment.
A droplet is 5-10 micrometers (µm). A micrometer is 1000 times larger than a micron (µ). Please recall COVID is about .1 µ. The motion of really large droplets 60-100 µm are governed by gravity. They quickly descend when released in a sneeze or a cough. These are droplets that are about the size of a dust particle on the small end, or about the width of a human hair on the large end.
Droplets that are generally associated with respiratory viruses are between 5-10 µ. Particles that are less than 5 µ can more easily infect the lower respiratory tract, while particles that are 6-12 µ generally are limited to the upper respiratory tract.
This data should have you questioning the value of the 6-foot rule recommended by the CDC. They did eventually admit that there was no data behind that decision.
Since these particles are so small, masking is almost useless and IH professionals know this to be true. Therefore, industrial or “engineering controls” that utilize destruction and dilution are the most effective way to deal with aerosol dispersion.
What are some examples of engineering controls for COVID-19?
Minimum Efficiency Reporting Value (MERV) ventilation with MERV 14 filters
Now that we understand the role of an IH, OSHA and EPA standards that provide protection against small aerosols, and the relative effectiveness associated with personal protective measures and engineering controls, we are ready to ask our employer a few more pointed questions.
Good day,
I would like to reach out to our organization’s industrial hygienists (IH) or others with similar responsibilities. I have additional questions related to masking mandates.
Please advise what engineering controls were implemented to mitigate the spread of respiratory viruses. I am particularly interested in determining if these industrial methods meet OSHA and EPA requirements.
Did we install Minimum Efficiency Reporting Value (MERV) ventilation with MERV 14 filters, High Efficiency Particulate Air (HEPA) filters, and Ultraviolet (UV) sterilization units?
If not, can you explain why? As you are aware, OSHA and the EPA have concluded that masking without a respirator has almost no value in preventing the spread of an aerosol. The most effective methods are engineering controls. It is important the workforce understand why these were not included as part of our employer’s mitigation plan.
If not, can you provide a cost differential analysis showing that the purchase of masks will be less costly than implementing more permanent engineering controls. These engineering controls would not require the same amount of repeated capital input, theoretically every flu season.
If they were implemented, what data supports masking and other personal protective measures will enhance the results? Our employer must maintain data, per OSHA guidelines, on the effectiveness of our organization’s IH-directed mitigation protocols. If masking were effective, then this would be reflected in the data collected by our IH as part of their duties defined by regulatory and statutory code.
Where can an employee find the data our IH has collected between 2020-2023 showing the effectiveness of mitigation measures employed by our organization? If it is not available, why? Will it be made available?
Has my union been provided all this information? If so, how did they respond?
With respect,
Employee Title and Name
Contact Information
Elected officials need to act.
I am sure you can identify additional lines of questioning that could be posed of your employer, and I encourage you to do so. Perhaps you could send a pointed letter asking if there is liability protection for any future deleterious health effects associated with long term mask usage. Given masking a healthy adult is an experimental medical intervention, perhaps you could ask them if they have provided a full list of side effects in the name of informed consent. I will leave that up to your imagination.
There are two more actions you can take to help protect you from illegal mask mandates.
Please write a letter to your State Attorney General (AG) and governor. Provide them with a detailed description of what is happening in your place of employment. Ask the governor to take executive action and express an interest in the AG exercising their power to litigate. I will be glad to provide example letters in a future Substack if there is interest.
Senators Mike Braun, J.D. Vance, and cosponsors Senator Josh Hawley and Eric Schmitt have introduced legislation (Freedom to Breath Act) to ban mask mandates for domestic travel, public transit systems, and primary, secondary, and post-secondary schools. I encourage you to write or call your representatives and have them support this legislation.
The next Substack in this series will be published in the next week, and it will provide you with all the data you need to shut down debate on mask mandates.
The opinions expressed are my own and do not reflect the opinions of the federal government (unfortunately), nor do they reflect the opinions of Feds for Freedom.