

Do masks work? They are a talisman.
Do masks work? They are a talisman.
Part 3: The Data

If you have followed my two other posts, and you aren’t that interested in the data, rest assured. You can read the first section of this Substack, and you will be armed with enough information to shut down most debate on masks.
Repeat the specifics to any mask devotee to let them know you will not be bullied into compliance. I strongly urge you to read part 1 of this series, as this will be the most effective means of influence; however, if your only goal is to embarrass institutionalized hypochondriacs for their stupidity, please just dive into the data.

Cochran study: After conducting a randomized controlled study with 276,000 participants, researchers found no benefit from societal use of masks. The lead researcher spoke to the press and said:
There is just no evidence that they make any difference. Full stop. My job, our job as a review team was to look at the evidence. We have done that. Not just for masks. We looked at hand washing sterilization, goggles, etc…
Dutch study: Dutch researchers reported on 18 November 2020 that surgical masks did not provide the wearer greater protection from SARS-CoV-2. The research was a thorough randomized, clinical study published in the Annals of Internal Medicine, and the first definitive scientific evidence indicating mask mandates were unnecessary.
The study did not dispute the supposition that masks prevented sick people from spreading the disease, but the study was not designed to investigate this type of transmission. It only focused on mask efficacy used by healthy participants.1
These studies make it hard for mask devotees to argue, but they will. You will hear all sorts of accusations and explanations, and they will cover a range of topics.
Everyone wasn’t wearing them right!
People are too stupid to know what’s good for them!
They need N95 masks!
Those studies are from right wing anti-vax nutters!
You are a racist!
So, they want us all in N95 or K95 masks? If you’re interested in the data, please continue reading.
But what about the N95? They told me I would be safe…
N95 respirators and surgical masks may have some benefit under specific and highly controlled conditions, and only for limited durations. They do not filter for particles the size of coronavirus. The only masks capable of reliably filtering for small viral particles are industrial respirators.
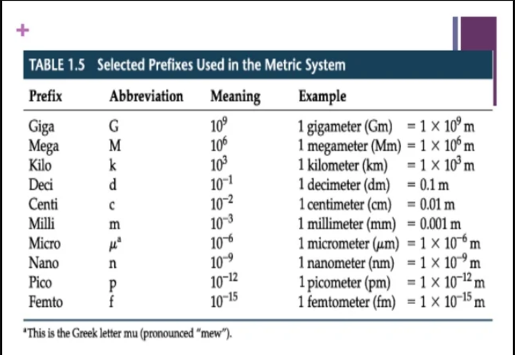
This Personal Protective Equipment (PPE) will protect you from particles smaller than .3 µ, are expensive, and generally used for chemical and biological contaminants that pose deadly near-term effects or debilitating long-term health problems.
Unfortunately, N95 respirators are only rated to filter for particles greater than .3 µ and they must be properly fitted to be effective.
Viral particles may be temporarily trapped on N95 and surgical masks due to the electrostatic potential of the fabric, and transmission may be further limited by other mitigation measures, but they are not a societal panacea.
Most studies showing a marginal benefit are conducted in a hospital setting that also includes engineering measures designed to limit transmission. These highly specific conditions resulting in potential benefit include rigorous secondary disinfection measures, frequent changing of properly fitted masks, and use of masks rated for protection against viruses (respirators); however, they are not useful in community wide mitigation measures.2
Health care workers wear them because they are more likely than the average person to be exposed to large droplets for a period sufficient to be infected. If N95 masks work, one could make the case for widespread public usage. A logical reason to wear masks, the reason which seems most understandable to the lay person, is that droplets carry the virus and the droplets that carry the virus can be stopped by a mask. Therefore, wearing a mask could serve to protect oneself and others.
This makes widespread usage appear superficially plausible. The problem is the binary rhetoric devoid of the nuance necessary to understand mask efficacy. The dialogue has been boiled down to masks work, so if you don’t wear them you are engaging in dangerous activity impacting everyone.
The government has propagated misinformation by taking the plausible, common-sense explanation that masks can be efficacious under certain rarefied conditions, while ignoring the fact that all studies focusing on societal usage have contradicted their public statements. The actions of the federal government have also been a matter of costly public policy.
Every government agency purchased millions of dollars worth of masks, and mask mandates forced private industry to purchase them too. DIY masks became a side hustle for many burgeoning entrepreneurs, and Indian suppliers of mask material made a fortune.
Chinese PPE producers also enjoyed a financial windfall, purchasing huge amounts of mask material in January and February 2020, while subsequently selling them for a profit. Despite the supply chain issues, and the difficulty getting China to open up its mask market, in January and February 2020 the US provided China with millions of dollars’ worth of face masks and protective equipment.
By late January, the US government was fully aware that there was the potential need for protective equipment at home.
Then the US purchased masks from China, the country partially responsible for the pandemic, while complaining about China’s response to… the pandemic. To make matters worse, China appeared to be purposely hoarding masks exactly when nations were clamoring for additional supplies.
None of it made sense.
Provide China with masks, then purchase masks from China? If I were a conspiracy theorist, I’d say it looks a lot like somebody in the US government had invested heavily in industries that support the mask and medical industry.
The policy cost wasn’t just confined to the purchase of PPE or other measures requiring significant capital investment. The second and third order effects have yet to be fully felt. Environmental clean-up associated with the huge number of discarded masks represent an unknown, but huge cost. Education loss and mental distress forced on our children will have devastating long term effects.
It didn’t matter that they didn’t work, and the mask madness makes one wonder… Why the hysteria? Many other writers have covered this subject ad nauseam, but in my opinion it was a little bit financial benefit and a little bit psyop.
Stop arguing… The science has been settled.
Masks were considered settled science, like many other topics surrounding C19. To speak otherwise was heretical in the new religion, where fear of a virus replaced fear of eternal damnation. It became a moral test.
Settled science is the antithesis of scientific inquiry. There is no single field of mask science for devotees to follow. This is exemplified when one looks at C19 knowledge gaps surrounding surface chemistry, aerosolized agents, infectious spread, biophysics of the infectious agent and fabric, and electrochemical properties of the biological material, as well as a whole host of other very complicated lines of research.
We know one thing for sure. Masks and respirators filter out unwanted material. The first step is understanding how filtration works.
Let’s filter out the nonsense…
There are six mechanisms associated with filtration of droplets and aerosols and they have variables independent and specific to each of them:
Filtration of larger particles is generally governed by gravity and sedimentation. Smaller particles are subject to the laws of Brownian motion and mechanical interception, while the smallest particles which measure below 100 nanometers (nm) (.1 µ) rely on electrostatic attraction for filtration efficacy. SARS-CoV-2 lies just below that .1 µ range.
Filtration is more efficient at low velocities, like breathing through a face mask, and every material has a different velocity thresh hold. If the force pushing air through the mask is too high, small water droplets are simply aerosolized, and pushed out the other side of the mask. Even the relatively weak force behind one’s respiration will eventually force water vapor through a mask, aerosolizing it in the process.
Brownian motion is a key concept one must understand when discussing the efficacy of masks, particularly in relation to SARS-CoV-2. Imagine a leaf caught in the cross winds of a small alley. The leaf has no discernable, predictable motion. It can remain suspended in the air for minutes or get trapped on the side of a building before being shot upwards out of sight. Even though the leaf is small in comparison to the buildings that limit its movement, the three-dimensional nature of the obstacles as compared to the relatively small dimensions of the leaf really don’t help to predict which leaves will escape and which will remain plastered against the “monitored-by-ADT” sign. It is random motion.
Well, I know the counter argument.
Masks prevent the larger droplets from infecting others, and it is better than nothing.
Well… It might make it worse…
If we dispense with the analogy and put our SARS-CoV-2 virus in physical context, we are talking about a virus around .1 µ in diameter, suspended in varying sizes of aerosolized water. The water ranges in size from 200 to 20000 µ in diameter; so multiple orders of magnitude larger than virus. The average diameter of a cotton thread is much thicker, and the gaps between those fibers are even wider.
Large droplets are primarily filtered through gravity, and droplets may temporarily be deposited on a mask. Absent a respirator, they are subject to forced filtration. As we breath, the droplets are forced through the mask and diminish in size. Counter-intuitively, this often results in a greater viral load for each aerosol-sized particle. Evaporation forces greater amounts of viral material into each water droplet.
Britannica describes the various methods of forced filtration aptly.
The fluid to be filtered will pass through the filter medium only if some driving force is applied. This force may be caused by gravity, centrifugation, application of pressure on the fluid above the filter, or application of vacuum below the filter or by a combination of such forces. Gravitational force alone may be used in large sand-bed filters and in simple laboratory filtrations. Centrifuges containing a bowl with a porous filter medium may be considered as filters in which gravitational force is replaced by centrifugal force many times greater than gravity. If a laboratory filtration is difficult a partial vacuum is usually applied to the container below the filter medium to increase the rate of filtration. Most industrial filtration processes involve the use of pressure or vacuum, depending upon the type of filter used, to increase the rate of filtration and to decrease the size of the equipment required.
If small viral particles suspended in liquid happen to be trapped by a mask’s fibers, it is primarily dependent upon the electrostatic attraction of that fiber and the vapor. This is not a permanent filtration solution when the mask is not rated to trap particles the size of SARS-CoV-2.
Let me reiterate, no more force than the natural rise and fall of one’s chest is necessary to further aerosolize SARS-CoV-2 lingering on one’s DIY mask.

In an enclosed temperature-controlled office environment, those aerosols can remain suspended in the air longer than the larger droplets which are falling harmlessly to the ground. Several studies have concluded that forced filtration increases aerosolization and the virus can stay suspended in the air nine hours.
Other studies that have not been reproduced claim that aerosols can remain suspended in the air in office environments for up to 30 hours. The jury is still out on the latter claims; however, it appears reasonable to assume aerosols can remain suspended throughout a normal workday. Masking therefore increases the capacity of the viral material to spread in an enclosed environment like an office.
Don’t worry too much though, a recent study shows that SARS-CoV-2 loses 90% its ability to infect after 20 minutes airborne. The point is, in addition to being an excellent bacterial breeding ground, masking in the office may actual produce many more infectious particles over an albeit shorter timeframe.
We’ve also always known that single stranded RNA viruses are fragile and degrade very quickly in UV light. You know… when the sun is out.
Some of the aerosolized infectious agent could be potentially be spread by release fomites and inhalation of these fibrous particles produced by cloth masks.
In one study exploring the efficacy of N95, surgical, and cloth masks, researchers were confounded by results showing an increase in aerosolized particles when using cloth masks. As one respires, aerosolized water and droplets either originating from the wearer or from others in proximity can land on the fibers of the mask.
It causes mask material to be released in small fibrous particles which are moist, warm habitats for viable viral agents and serve as a solid structure by which mucosal material and viral material can comfortably interact.
The peer-reviewed study raised the distinct possibility that cloth masks were not only ineffective, but potentially deleteriously amplifying the spread of infectious agent. The only solution researchers presented to address the problem included use of N95 and surgical masks that were changed multiple times over the course of very short periods of time.3
Does this seem like a commonsense approach to societal level mitigation measures?
In simpler terms, since C19 is airborne, and the commercially available masks only filter to a maximum of 4 µ, then masks will either not catch the particle or make the particles smaller. A virus isn’t a solid, immutable material, nor is water. If you have a strainer and pour water into it, it doesn’t matter how small the holes are in the strainer, water comes out the other end. Even if you reduce the size of the openings in your strainer, water still comes out.
When those holes get small enough, electrostatic attraction will hold the water in the mouth of the hole’s opening by surface tension; these are factors arising from the electrochemical properties of water (and the strainer). In this case, the strainer would have a moist look, but even a very small movement would cause much smaller water droplets to shake loose.
A sneeze – which is often called ballistic respiration – would shake loose even more. The studies cited note that natural respiration is sufficient to force the droplets through a mask.
SARS-CoV-2 measures about .1 µ. During ballistic respiration from a sneeze or cough, only particles larger than 4 µ are caught. The rest is pushed through the mask via forced filtration, in some cases the droplets are reduced in size as it is filtered through the mask, and left suspended in the air, subject only to the whims of Brownian motion.
Get it? It doesn’t work.
Electrostatic potential is a temporary fix …
Various fabrics have different electrostatic capacities, and variations on the type of multiple distinct layers of cloth in masks have shown increased efficacy against transmission of aerosolized water. The electric charge of the fabric is important.
Water is electronegative, meaning H2O tends to want to attract electrons. Fabric can “store up” excess electrons and this is what causes the water to attract to the threads of fabric. The charge in fabric is malleable as electrons are stored up and released, and the electrons are moving, so water vapor is never permanently attached to any part of the mask. The water can be freed and recaptured depending on the environment.
It is a random phenomenon. We will have a very hard time predicting just how much transmission will be reduced when using these masks.
Throughout the 2009 H1N1 pandemic, the west African Ebola Pandemic of 2014, and SARS and MERS epidemics, guidelines by the WHO, the CDC, and European health agencies have been consistent on the value of social distancing, but there has been - at best - conflicting guidance on mask usage. The science is complicated and there is an obvious reason studies have concluded masks are only recommended for hospital settings where there is an identified risk, in a closely controlled environment.
Even social distancing has conflicting guidance, depending on the mode of transmission of the viral or bacterial agent. For example, Ebola is passed by bodily fluid exchange. Social distancing is a key measure.
Why is there so much conflicting guidance?
Conflicting guidance
The WHO, the US Surgeon General Jerome Adams, and Dr. Anthony Fauci advised against widespread use of masks at the outset of the C19 pandemic chaos. They eventually changed their minds without providing any proof of the potential benefits.
Dr. Fauci advised that it was to ensure health professionals would have access to limited supplies of N95 and surgical masks if the public began hysterically purchasing pandemic supplies.

European health officials like Denmark’s Rigshospitale chief physician Henning Bundgaard resisted the use of masks and publicly stated that all countries using masks were making their decisions based on new studies that did not show a medical effect from wearing a mask. He authored a study that found a slight benefit of mask wearing but clarified that the study’s results only assessed the use of masks as personal protection, not source protection.
This was an observational study that showed a .03% difference between the masked and unmasked population. The backtracking had the hallmarks of a public health official under attack from consensus science.
Denmark’s Coen Berends, a spokesman for the National Institute for Public Health and the Environment and the Medical Minister Tamara van Ark agreed that there was a lack of sound science and evidence of effectiveness. Sweden’s top infectious disease expert, Anders Tengell, also agreed and added that masks were not useful on public transportation.
A WHO-supported analysis of 10 randomized controlled trials (RCT)4 ultimately did not support the efficacy of medical masks, hand hygiene, and surface and object cleaning in social settings, because they could not reduce infection rates of some viral respiratory diseases. The study also emphasized this conclusion applied to source control for the infected and healthy participants in the study.
“…masks worn by the infected person for source control OR when worn by uninfected persons.”
21 mask studies identified by specific search sequences in 12 scientific search engines and an additional 25 laboratory publications examining the prevention of transmission of droplet and aerosol spread agents were reviewed by researchers. All the studies used medium or low-level evidence designs with most of the studies having important unexplainable impact as a result of bundling of other infectious disease control measures. Because of the paucity of high-quality studies in healthcare settings, the advocacy of all mask types was not assessed to be entirely evidence based. It did, however, conclude that a 1-meter respiratory zone might need expansion and N95 masks did offer greater protection against viral sized particles in a hospital setting.5
A relevant randomized controlled mask study looking at the spread of influenza virus found masks ineffective. SARS-CoV-2 is physically larger than influenza, so while not directly relatable, it is a worthy datapoint.6
As of 12 February 2020, the CDC did not recommend the use of a mask only stating that they did not consider C19 sufficiently prevalent in the community to warrant such guidance. It was only recommended if one was sick or was in contact with an individual who may be sick, or at a health care office.7
In March and April of 2020 there was conflicting scientific discourse on the effectiveness of DIY masks, and concern that they provided a false sense of security that represented a potential moral hazard; the mask could cause people to engage in risky behavior because they felt as though they were safe.
By May of 2020, CDC provided guidance advising the use of cloth face masks as a voluntary measure in very specific higher risk circumstances. Some medical professionals commented that it was a matter of ensuring there was sufficient N95 and surgical masks for medical professionals. Others noted that it was predicated on the prevention of pre-symptomatic and asymptomatic spread, of which little was known at that time.8
Not too long after, masks became mandated using asymptomatic spread as one of the justifications. CDC fully reversed course by late July 2020 after of a review of a case study and an editorial from JAMA which claimed to show universal masking reduced spread.9 It described conditions in a hospital environment, was not a randomized clinical trial, and did not examine the potential for widespread societal level use of masking.
The other was a case study surrounding a Missouri hair salon’s experience with C19, and a review of CDC’s Morbidity and Mortality Weekly Report (MMWR), which allegedly showed a correlation between mask usage and reduction in spread of C19. This was not peer-reviewed science or deep investigations into cloth fabric efficacy. It was anecdotal science, which has since proven to be completely unsubstantiated by the growing body of evidence contradicting this point-in-time case study.10
Is this what CDC thinks constitutes sufficient science to warrant a policy which has had dramatic social and economic consequences?
Asymptomatic spread …
Asymptomatic spread was just one of a number of scare tactics meant to coerce the public into compliance. We knew in 2020 that asymptomatic spread was never a driver of pandemics.
In September 2020, Fauci made a scientifically accurate statement about asymptomatic spread. The video has been scrubbed from the search engines, but I did manage to find a link on Startpage.com.
“The one thing historically people have to realize… in all the history of respiratory borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks, the driver of outbreaks is always a symptomatic person, even if there is a rare asymptomatic person that might transmit an epidemic is not driven by asymptomatic carriers.”
In June 2020, the who said that asymptomatic spread was “very rare.”
The WHO technical lead Maria Van Kerkhove must have experienced a significant degree of backlash from individuals invested in the consensus science narrative, because she clarified the “very rare” statement one day later emphasizing the variable results of asymptomatic studies. She carefully adjusted her language to reflect:
“…data from member countries suggest that asymptomatic individuals are much less likely to transmit the virus.”
Outside experts and WHO officials have acknowledged that detecting asymptomatic spread is challenging. Some of these experts comment that just because scientists haven’t seen something occurring, doesn’t mean it’s not happening. We are forced to prove a negative. Scientists aren’t seeing it, but prove it isn’t happening.11
The National Center for Immunization Research and Surveillance in Australia contact-traced 18 infected students and faculty between March and April 2020, through 862 close contacts spanning 15 schools. Close contact was defined as 15 minutes of face-to-face continuous contact or in the same room for two hours with an infected person. Those in close contact were tested (735 students and 128 staff members) and only 2 infections were identified. A transmission rate of .2% in active social settings in a school without masks makes any conclusions related to mask mandates or asymptomatic spread appear patently absurd.12
In a separate study,13 14 randomized control studies in hospital settings showed that cloth masks did not provide protection from viral infection. It looked at 1607 medical care workers to determine if cloth masks led to higher respiratory infection rates. It concluded that the rate of influenza-like illness was statistically higher. Although speculative in nature, the study commented:
“Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
What is certain? Even if we discount Dr. Fauci’s statements in September 2020, by at least April of 2021, CDC knew that asymptomatic spread was almost nonexistent.
One comprehensive study coming out of the C19 epidemic epicenter, Wuhan, China, resulted in findings that appeared to indicate asymptomatic spread was not a risk. “A mass screening of more than 10 million residents of Wuhan, China, performed after SARS-CoV-2 was brought under control, only identified 300 cases that were not infectious.14
Since then, we have all seen misinformationists work overtime to try and provide additional scientific backing post-script. Do you think these policy makers want to admit they made a mistake? Do you think the bureaucrats may have incentive to lean in on more oppressive policies or color the science to cover up their bumbling incompetence?
Fauci admits they don’t work on a societal level.
Yeah, but there are other studies, Michael, that show at an individual level for an individual when you’re talking about the effect on the epidemic or the pandemic as a whole, the data are less strong, but when you talk about as an individual basis of someone protecting themselves or protecting themselves from spreading it to others, there is no doubt that there are many studies that show that there is an advantage.
Regardless of the mixed messages, the few valid attempts to explore masking has had significant scientific problems.
Getting Deep into the data.
If you have been reading this long, even if the specific data is not your cup of tea, you might as well sit back, take a sip, and read the details.
There are some fundamental studies that need additional data and research examining material performance, environmental factors, and potential adverse effects.
Let me emphasize that the research is generally sound from an initial point of scientific inquiry standpoint, but the measures that would have to be undertaken at a societal level are generally not realistic, and the methods are crude.
Like any good science, the studies looking at a very specific issue and control for micro-environmental variables; however, one cannot extrapolate those results and make predictions about what we will see on the macro, societal level. Human action is not predictable nor controllable.
Most studies do not consider mask leakage, or if they do test for leakage, it is a “systematic, controlled leakage”. This sort of testing is required to help in the scientific process and is a necessary step in building a knowledge base; however, leaks are a random occurrence which will result in a random expulsion of a random amount of water vapor carrying a random amount of protein-wrapped viral genetic material.
Environmental factors like humidity and temperature will have a large effect on homemade masks but this factor was not explored in most studies. More important, even minor gaps in fitting caused large decreases in efficiency in all materials.
If data is limited, one side will argue what is the harm in just wearing a cloth mask substitute given the lack of N95 respirator grade masks.
The same argument can be made from the other side. What science supports forcing healthy individuals to engage in activity that has not fully explored second order health effects nor fully proven that engaging in the activity will have the desired health benefit results?
Why wear a mask when it has a potential negative effect on herd immunity? The young and healthy are at extraordinarily low risk.
Why wear a mask if asymptomatic spread has never been a key factor in transmission? Asymptomatic spread, as Fauci previously stated, has never been a main driver of pandemics.
Why wear a mask if there are known adverse side effects? There are now studies showing toxic chemicals in the masks, fomite build-up in the lower lungs, and deleterious CO2 build-up.
Why make mask mandates if it has never been part of an effective nationwide strategy and when there have been many opportunities to prove its value during the dozen or so epidemics over the last century? Knowing that only a small portion of the population is in danger from C19, then why is it not reasonable to ask only those most at risk, and those who believe they need to wear a mask, to do so? Why can’t we just have those at risk undertake protective measures, and leave everyone else alone?
In general terms, the science being used to justify mask mandates included poor observational studies and misinterpretation of poorly constructed trials. The specifics are important to understand. The most important data related issues that call into question the use of masks include:
Use of crude, non-standardized method, and theoretical mechanistic analysis even though they are exploring complex biological systems.
Uncertainty in spatial scale of transmission via droplet, spray, and aerosol inhalation, and contact spread.
Failure to examine the efficiency of cloth face coverings, while emphasizing value of respirators and surgical masks.
Studies are based on computer models lacking practical application, testing, and sufficient empirical data.
Anecdotal stories or non-scientific surveys that are not quantifiable.
Hypothetical contra factual scenarios, forcing the public to prove a negative.
Masking harms not adequately explored.
Crude methods and mechanistic analysis
Some of the studies use crude, non-standardized methods, and theoretical mechanistic analysis even though they are exploring complex biological systems.15161718
While some of these studies did show homemade cloth masks could be effective in blocking viral transmission, the problem with the results were apparent when we look at transmission data, neatly summarized by Tom Woods with a series of graphs.
There is no correlation between mask mandates and reduction in C19 spread. This could be a result of the multiple other potential variables that one is faced with when experimental controlled results are compared to societal application of health policy.
When examining fabric performance as a function of particle size and the effect of hybrid multi-layer methods to control transmission, most studies utilized an extremely mechanistic approach not found in biological systems.19
The research from Ma et al. from the College of Veterinary Medicine, Qingdao Agriculture University is often used to justify mask usage and frequent hand washing. Masks and hand washing are, as I stated previously, a “seemingly” common-sense approach to reducing viral spread and it is easy to get behind positive test results.
This research showed the benefit of hand washing in combination with wearing specific types of masks in reducing viral spread; however, the method used a closed nebulizer system that did not account for poor fitting masks, and the results required immediate hand-washing post viral exposure, which is obviously not a realistic response in most situations.
As you may recall from the second Substack in the mask series, properly fitted masks are a requirement to stop infection and transmission and is also an OSHA requirement for respirators.

One model key to understanding the ability of aerosolized particles to penetrate fibrous material examined the particle size range that fell between that of filtration by inertial impaction and Brownian motion. This is considered the sweet spot where filtration is at its least effective.
Particle velocity was also a key factor and as suspected, the faster the particle flow, the more particles of smaller size capable of passing through the filter. The mechanistic model was good at predicting filtration particle size at speeds of 100 cm per second or less; however, the experimental and theoretical results had significant divergence at higher velocities.20 A sneeze is about 4470.4 centimeters per second. Breathing velocity ranges between 60 and 140 cm per second.21
One study attempted to explore the role of the electrostatic charge in N99, N95, and P100 filters. Once again, the method used to strip the charge was accomplished through chemical means. This degraded filtration efficacy, allowing for larger sized particles to pass through the filter.22
Given that all cloth material has an electrostatic charge, it is variable, and can change during wear, this study could potentially validate claims regarding the efficacy of home-made masks. That said, the method for eliminating the charge was not one found in a natural setting, and the masks being tested did not include the kinds being utilized to stop the spread of C19.
A study from the New England Journal of Medicine used a collision nebulizer to simulate coughing and sneezing. The results were largely misinterpreted by the media and news outlets like the New York Times, Reuters, and the British Broadcasting Company (BBC) claimed that the result showed viral material could remain viable in aerosolized water for up to three hours.
This was a serious misunderstanding as to the difference between clinical and test conditions. Another misunderstanding was related to conditions for survival of viral material in open air; they made assumptions based on extrapolations from testing in strictly controlled environments, vice open air conditions.23
Another study repurposed a metered-dose inhaler to generate fluorescent-tagged droplets at specific velocities mimicking human breathing and ballistic speeds mimicking sneezing and coughing. It allowed the researchers to quantify blocking capacity of various fabrics and it did show that cloth masks could be effective in blocking viral transmission.
The process was once again “ a highly mechanistic process” that had mixed results and qualifications. The study noted that homemade masks of any cloth variety also held water and, in some cases, viable viral material longer. It also emphasized the need for several other measures to be used in conjunction with masks.24
Some of these studies were good science25, in so far as they were also willing to directly identify the gaps in their research.
Thus any mask, no matter how efficient at filtration or how good the seal, will have minimal effect if it is not used in conjunction with other preventative measures, such as isolation of infected cases, immunization, good respiratory etiquette, and regular hand hygiene…these masks would provide the wearer little protection from microorganisms from other persons who are infected with respiratory diseases. As a result, we would not recommend homemade masks as a method of reducing transmission from infected aerosols.
Uncertainty in spatial scale and transmission
There is still a great deal of uncertainty in the role and spatial scale for transmission via droplet, spray, aerosol inhalation, or contact for respiratory diseases including C19.
Neither the aerosol viral load nor the minimum infectious dose for C19 have been definitively established. We don’t know the viability of C19 in aerosolized particles but can assume that a virus with a full protein shell could still be infectious. The mode of transmission would appear to be through droplets, possibly through aerosolized water, and through direct contact.
Researchers have conducted a variety of detailed analyses and studies;2627 however, they have often been misinterpreted and extrapolated into meanings that go beyond the experimental setting and have led the media to make broad clinical leaps of faith.
One study meant to explore the tenacity and stability of SARS-CoV-2 with SARS-CoV-1 as a comparison on surfaces and in aerosols, concluded SARS-CoV-2 could be spread by droplets (larger) and despite N95 mask usage in a hospital setting, it was found to have spread via contact. It matched previous WHO reporting that concluded there was far less likelihood of aerosolized spread of the disease. Social distancing should be enough to stem the spread of the disease.28
More research is needed, but the research we do have can lead us to the conclusion that little is known about SARS-CoV-2 transmission. Social distancing may be a good means of protecting oneself from infection; however, aerosolized SARS-CoV-2 won’t adhere to the six-foot rule.
The results potentially indicate that aggressive use of properly fitted masks and secondary health measures like frequent hand-washing and changing of masks could be effective, but only if a strict protocol were held by every individual engaging in the activity and it only showed effectiveness in health care environments.293031
One meta-analysis of 10 studies discussed even more unrealistic social distancing, suggesting up to 8 meters for droplet transmission. Droplets are produced in coughing and sneezing, and the average person normally takes measures to not spray their bodily fluids eight meters. The meta-analysis also commented that SARS-CoV-2 aerosolized agent could be found in the air for as long as 3 hours after becoming an aerosol.
The viability and viral load were unknown, and the methods were once again, not instructive for social settings. Furthermore, it cast doubt on the ability to neatly separate between droplet and aerosol spread of the disease. It concluded by stating that the combined evidence supported airborne precautions for the occupational health and safety of health workers treating patients with COVID-19.32
The CDC’s defense of cloth masks included one study in which multi-layer cloth was assessed to help block 50-70 percent of fine droplets. They elaborated by saying that 20 to 50 percent of fine particles made it through the mask, and minimal viral load is required – especially if aerosolized – in order to transmit C19. There were no control variables, and it was limited to observational and epidemiological studies. (Centers for Disease Control, 2020)
What about the cloth masks?
Most studies are not relevant because they examined the efficiency of respirators and surgical masks but did not investigate efficacy of cloth face coverings.
Until N95 masks can be mass-produced affordably, and personal habits are changed on a societal level, this is an unrealistic proposition. Additionally, only industrial respirators are rated to filter contaminants the size of SARS-CoV-2.
There is a body of literature surrounding the efficacy of surgical masks and there are studies that show some efficacy under very specific conditions. There earliest studies were from the field of dentistry, and surgical masks were intended to protect the patient from any inadvertent transfer of bodily fluids (like blood) between the patient and health care workers. Much later, masks were introduced to assist in protecting health care workers from infectious disease.
One of the studies showed that there was a decrease in the detection of viral particles in respiratory droplets and aerosols when a surgical mask was in use; however, scientists only detected coronavirus in 4 of 10 unmasked people infected with coronavirus, the viral load was very low, and they could not confirm that the viral particles detected by rtPCR were viable or capable of infecting others. Therefore, the conclusion to the limited scope study could only state definitively that people known to be infected may limit transmission through use of a surgical mask.33
In another study, both surgical and N95 masks were effective when used for short periods to prevent the spread of infection from actively sick individuals. This was a limited scope study that has not been reproduced, using nonbiological particles. It did not test for positive PCR results, and only measured positive point of care assay results. The study did not prove that viral material captured by the masks were in fact contagious. Additionally, the study only looked at 3-5 minutes of mask use and there was no way to know if long-term mask use would be as efficacious.34
Five types of commercially available surgical masks were tested for their ability to arrest infectious agents using a nebulizer set-up and mannequins. It looked closely at the ability of the masks to stop aerosolized bioagent. Mean values of bioaerosol arrest were at about 48-68%; however, as noted above, this was in a laboratory environment and was only tested for short term use.35
Computer models and empirical data.
Many studies are based on computer models that do not have sound practical application, testing, or sufficient empirical data.
There have been many examples of poorly constructed computer models. I wrote about one in a previous Substack.

One study estimated the prevalence of contagious, asymptomatic spread using models of data coming from China early during the pandemic. The study was observational data combined with mobility data, a networked metapopulation model, and Bayesian inference to determine the percentage of asymptomatic carriers.
Even if one were to ignore that the original data set is from China, we would have to all agree that 86% were asymptomatic carriers.36 Seems like an absurd number not matched by any other statistical analysis.
One model key to understanding the propagation of aerosolized material required test subjects to cough into a box, tube, or specified space. Follow up work from the same researcher used different techniques to examine air flow, validating data from the previous study in a more natural setting, but it was still confined to a controlled environment. Droplet and aerosol propagation could not be translated into viral spread for SARS-CoV-2. There was a great deal of variability on test subject responses, in terms of the shape of the mouth during coughing, droplets expelled during sneezing, and velocities.3738
Save your stories for the library’s fiction section.
Many studies and media reports masquerading as science are based on anecdotal stories or non-scientific surveys that are not quantifiable.
One paper submitted a series of anecdotal stories used to justify aerosols as an important means of viral contagion. One supposition for the limited spread of disease in hospital environments gave credit to superior ventilation systems. I believe this to be a good assumption, but the studies to support the claim have not been conducted.39
Many have cited a chorale recital in Skagit Valley, Washington as an example of the need for masks. Two members of the chorale ended up dying of C19, while 45 became ill. The median age of those attending chorale practice were 69, three were hospitalized and had two or more underlying conditions. Of those three that were hospitalized, two died. They were aged 80 and 83. 4041
This tragedy is an example of the need to protect the most vulnerable segments of the population, vice a ringing endorsement of mask policies. What is especially sad is how the media has turned this great loss into an excuse to ridicule these people for their religious beliefs and their desire to engage in activity that gives their lives value.

Another key anecdotal study focused on an airborne outbreak at a restaurant in Guangzhou, China where ten diners contracted SARS-CoV-2. Again, the story was used to emphasize the possibility of aerosolized spread of the disease. It did not result in the death of those infected and they all recovered.
The research also had several glaring flaws. There was no real hypothesis stated, the use of chi-sq test was not clearly defined, causality and statistical significance was not fully established.4243
One paper was written following the 2003 SARS epidemic.44 It is often used as reference material for why we need to mask up, but these honest articles fail to tell you what the paper actually says.
The article points out that there was no way to determine if masks were effective, but the voluntarily enforced guidelines may have served to raise awareness and incentivize good health practices.45
SARS has been called the first global epidemic of the 21st century and has been the cause of a massive and varied public health response in many countries of the world. This report describes observations made by two authors on a journey from Manchester in the United Kingdom to Chiang Mai in Thailand during the peak of global transmission. The public response to SARS, particularly characterized by the wearing of face masks, seemed to outstrip official guidance. Though of uncertain protective benefit, the wearing of masks may have contributed to the awareness of the collective and personal responsibility in combating infectious disease. Active and empowered involvement of the general public in implementing and cooperating with public health control measures supported by national and international authorities has clearly helped to bring SARS under control. The public health significance of such potent symbols as the face mask may be considered in strategies to tackle other emerging infections.
Masks kept millions out of the hospital! Prove me wrong.
The arguments often include hypothetical contra factual scenarios, which force the reader to prove a negative.
An article in Health Affairs is probably the best example of the fiction involved in the alleged research. This article examined mask polices from a few different localities and tried to show a statistically significant reduction in cases as a result of mask mandates. Graphs linked above, will disabuse the reader of the effectiveness of mask mandates; however, what was telling was exactly how the authors framed the discussion.
They claim that mask mandates avoided 200,000 C19 cases. There is no way to prove that it is true; however, those who wish to argue against mandatory masks, must argue why the policies didn’t save 200,000 lives.46
These often have limited scope surveys, where they draw a correlation between a localized reduction in cases and mask mandates. There are a variety of reasons cases could reduce in number. The natural Hope-Simpson curve, cross T-cell immunity, and maybe even severe lockdown measures represent plausible reasons.
A key example is a Hong Kong based study which was conducting comparative analysis.47 None of the other factors affecting a reduction in cases were considered, and broad conclusions were drawn based solely on the use or lack thereof of masks.
A lot of people are touting a study from the New England Journal of Medicine (NEJM) investigating droplet size of aerosolized water during normal speech with and without a mask, in comparison to coughing and sneezing. While some broad generalizations can be made about mask efficacy, and the need for proper fitting, additional PPE measures, and consistent application of health and safety measures (i.e. don’t touch your face, or use your mask to open door handles), you can’t make any broad generalizations regarding the spread of SARS-CoV-2.48
Here is the problem with folks like me who want a more thorough analysis of the mask science, and I don’t think it is one we can easily get around. A good study would be unethical. Masking healthy people and children and exposing them to a virus is unethical and potentially harmful as well… And I am not referring to the virus.
Masking harms have not been adequately addressed.
A quick read of some of the literature and it is reasonable to assume that there are some second order effects associated with mask usage, some of which may be harmful, that have not been fully explored and studied.
In 2023 the CDC finally admitted that mask usage can increase CO2 build-up, and it could result in deleterious health effects.
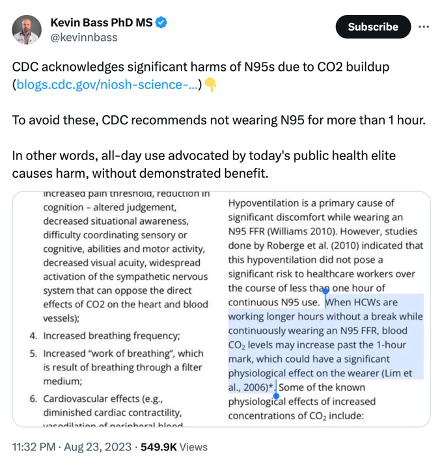
One study was particularly specific in the particular harms caused by mask mediated CO2 build-up. CO2 4.7 to 10.7 times higher than minimum toxic level.
Fresh air has around 0.04% CO2, while wearing masks more than 5 min bears a possible chronic exposure to carbon dioxide of 1.41% to 3.2% of the inhaled air. US Navy toxicity experts set the exposure limits for submarines carrying a female crew to 0.8% CO2 based on animal studies which indicated an increased risk for stillbirths. Additionally, mammals who were chronically exposed to 0.3% CO2 the experimental data demonstrate a teratogenicity with irreversible neuron damage in the offspring, reduced spatial learning caused by brainstem neuron apoptosis and reduced circulating levels of the insulin-like growth factor-1. With significant impact on three readout parameters (morphological, functional, marker) this chronic 0.3% CO2 exposure has to be defined as being toxic. Additional data exists on the exposure of chronic 0.3% CO2 in adolescent mammals causing neuron destruction, which includes less activity, increased anxiety and impaired learning and memory. There is also data indicating testicular toxicity in adolescents at CO2 inhalation concentrations above 0.5%.
Another study described a condition called Mask Induced Exhaustion Syndrome (MIES).
For a quantitative evaluation, 44 mostly experimental studies were referenced, and for a substantive evaluation, 65 publications were found. The literature revealed relevant adverse effects of masks in numerous disciplines. In this paper, we refer to the psychological and physical deterioration as well as multiple symptoms described because of their consistent, recurrent and uniform presentation from different disciplines as a MIES. We objectified evaluation evidenced changes in respiratory physiology of mask wearers with significant correlation of O2 drop and fatigue (p < 0.05), a clustered co-occurrence of respiratory impairment and O2 drop (67%), N95 mask and CO2 rise (82%), N95 mask and O2 drop (72%), N95 mask and headache (60%), respiratory impairment and temperature rise (88%), but also temperature rise and moisture (100%) under the masks. Extended mask-wearing by the general population could lead to relevant effects and consequences in many medical fields.
If we are breathing in fibrous material for months on end, I think it is reasonable to take a quick look at the types of ailments many in the textile industry suffer from. Byssinosis is the term used to describe an asthma-like set of symptoms associated with long-term exposure to organic textile dust contaminated with endotoxin, a component found on the cell wall of gram-negative bacteria. This bacterium is an extremely common contaminant of cotton.
Try not to worry… Any inadvertent decline in lung function is partially reversible.4950 One study concluded that long-term exposure to cotton dust, in which airborne endotoxin appears to play a role, results in substantial adverse chronic respiratory effects.51
Over 8000 chemicals are used to make textiles and some of the chemicals applied to our home-made masks may also contribute to cancer. There have been allergic responses to dyes which include eczema, urticaria, and asthma.525354Infertility in men and women has been tied to exposure to chemicals used in the textile industry.55
A search of peer-reviewed literature revealedf 54 relevant, published scientific papers linked textile industry worker exposure to a number of chemicals known to have carcinogenic properties with potential adverse long-term effects such as occupational cancer. These included breast cancer, biliary tract cancer, lung cancer, gastrointestinal cancer, colorectal cancer, and bladder cancer.56
I am sure those Chinese made masks are safe… no worries, right? Only the safest free-range, grass fed, organic dyes for your respiratory pleasure…
A mask study published by NIH suggests N95 Covid masks may expose wearers to dangerous level of toxic compounds linked to seizures and cancer. The Daily Mail wrote on 27 August 2023:
A study published in April found disposable masks can have toxic chemicals. Experts said this could make newly instated mask mandates ineffective. A study quietly re-shared by the National Institutes of Health in spring suggests the tight-fitting mask may expose users to dangerous levels of toxic chemicals. Researchers from Jeonbuk National University in South Korea looked at two types of disposable medical-grade masks, as well as several reusable cotton masks. The study found that the chemicals released by these masks had eight times the recommended safety limit of toxic volatile organic compounds (TVOCs). Inhaling TVOCs has been linked to health issues like headaches and nausea, while prolonged and repeated has been linked to organ damage and even cancer.

Forget an adults discomfort? Do you want your child breathing that stuff all day long… or even part of a day?
While assuming that the masks can serve as a psychological reminder to others to do the right thing and “mask-up.” One must also acknowledge that even the most devoted mask advocates encounter policy fatigue and, in some cases, passive resistance.
We don’t know – yet – if masks are causing harm, but that is sort of the point. No one cares to take it into consideration. Look up candida infections, or the effects of oral bacteria linked to heart disease and cancer that are normally expelled throughout the course of the day and tell me we know enough about “masking up” to ensure the second order effects of healthy people wearing masks are worth the risks.
More data that should make you think…
I have covered a lot of ground, but believe it or not, there is a LOT more data calling into question the value of masks in preventing respiratory infections.
The goal posts keep changing and supposed health experts keep changing their opinion. It is one thing to come to a new conclusion after a confluence of data and studies begin to point to new ways of doing things. The WHO and CDC and Dr. Fauci began the approach to this epidemic emphasizing that there was no need for masks, and then reversed themselves on the issue.
What changed in the matter of weeks? It certainly wasn’t new comprehensive studies on the issue. If anything, the studies have only further muddied the case for and against face masks.
It is hard to establish sound data on endemic, seasonal respiratory viruses prone to mutation. To really analyze transmission there would have to be one group that wears masks and are exposed to a virus and another group that does not wear masks and is exposed to a virus. As of 2006, no form of face covering had been tested for its effectiveness against influenza viruses.
Societal level measures have to be practical for everyone and easy to implement. A telephone news conference held 27 April 2006, hosted by the Institute of Medicine, Board on Health Sciences Policy, determined that there was no simple, reliable way to reuse disposable medical masks and N95 respirators. There is no process to dispense with fit testing, which is the only way to make them function properly. The committee was also hesitant to conclude that washable, woven masks should not be used; however, they cautioned that they were not likely as effective and could give a false sense of security leading to higher risk behavior.57
We have to contend with the possible negative downstream effects associated with implementing a measure that we know may not be effective, but might make people feel better.

Our policy makers and bureaucrats have to stop lying to us.
During a 16 September 2020 briefing to the U.S. Senate Appropriations Subcommittee hearing, the CDC director further exacerbated the moral hazard of a false sense of security by stating that masks are more effective against the virus than a future vaccine. It isn’t a ringing endorsement for vaccines, and it defies all known medical science, but remember he is an expert, and we should listen and remain silent.
Those people paid by the NIH to conduct the studies need to stop lying too.
One study supporting the efficacy of mask usage was retracted after statistics in the United States were showing a clear lack of correlation between mask usage and decreased levels of pathogen spread and hospitalizations.58 There are growing calls to have the Andersen et al. paper recalled as well.

How do we make a determination under these circumstances? The New England Journal of Medicine drew a pretty good conclusion.59
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to C19 as face-to-face contact within 6 feet with a patient with symptomatic. C19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching C19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
New England Journal of Medicine, 2020, 382,363
Bundgaard, Bundgarrd, Pedersen, Buchwald, Todsen, Norsk, . . . Iversen. (2020, November 18). Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers, A Randomized Controlled Trial. Annals of Internal Medicine, 10(7326).
Krouse, P. (2020, November 11). High quality N95 masks not practical for widespread use in controlling the spread of coronavirus. Retrieved from cleveland.com: https://www.cleveland.com/news/2020/11/high-quality-n-95-masks-not-practical-for-widespread-use-in-controlling-the-spread-of-coronavirus.html
Asadi, Cappa, Barreda, Wexler, Bouvier, & Ristenpart. (2020, 24 September). Efficacy of masks and face coverings in controlling outward aerosol particle emission from expiratory activities. Scientific Reports, 10(15665).
Xiao, Shiu, Gao, Wong, Fong, Ryu, & Cowling. (2020, May). Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings - personal Protective and Environmental Measures. Emerging Infectious Diseases, 26(5), 967-975.
Gralton, & McLaws. (2010, February). Protecting healthcare workers from pandemic: N95 or surgical masks? PubMed, 38(2), 657-67.
Xiao, Shiu, Gao, Wong, Fong, Ryu, & Cowling. (2020, May). Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings - personal Protective and Environmental Measures. Emerging Infectious Diseases, 26(5), 967-975.
Messonnier, D. N. (2020, February 12). Director of CDC's National Center for Immunization and Respiratory Diseases. (B. Hayes, Interviewer)
Bai, N. (2020, June 26). Still Confused About Face masks? Here's the Science Behind How Face Masks Prevent Coronavirus. Retrieved from UCSF: https://www.ucsf.edu/news/2020/06/417906/still-confused-about-masks-heres-science-behind-how-face-masks-prevent
Brooks, Butler, & Redfield. (2020, July 14). Universal Masking to Prevent SARS-CoV-2 Transmission - The Time is Now. JAMA, 324(7), 635-637.
Hendrix, Walde, Findley, & Trotman. (2020, July 17). Absence of Apparent Transmission of SARS-CoV-2 from Two Stylists After Exposure at a Hair Salon with a Universal Face Covering Policy - Springfield, Missouri, May 2020. Morbidity and Mortality Weekly Report, 69(28), 930-932.
Joseph, A. (2020, June 9). We don't actually have the answer yet": WHO clarifies comments on asymptomatic spread of Covid-19. Retrieved from STAT: https://www.statnews.com/2020/06/09/who-comments-asymptomatic-spread-covid-19/
Robertson, M. (2020, May 5). Why I'm Not Wearing a Mask. Retrieved from California Globe: https://californiaglobe.com/section-2/why-im-not-wearing-a-mask/?fbclid=IwAR3JDo7Um-HCq6AJnixCB2UT2UTc9T-HPTTrzcVWthL75f1-KiCiqbQerh8
MacIntyre, Seale, Dung, Hien, Nga, Chughtai, . . . Wang. (2020, April 22). A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. MBJ journals, 5(4).
Cao, Gan, Wang, Bachmann, Wei, Gong, . . . Lu. (2020, November 20). Post-lockdown SARS-CoV-2 nucleaic acid screening in nearly ten million residents of Wuhan, China. Nature Communications, 11(5917).
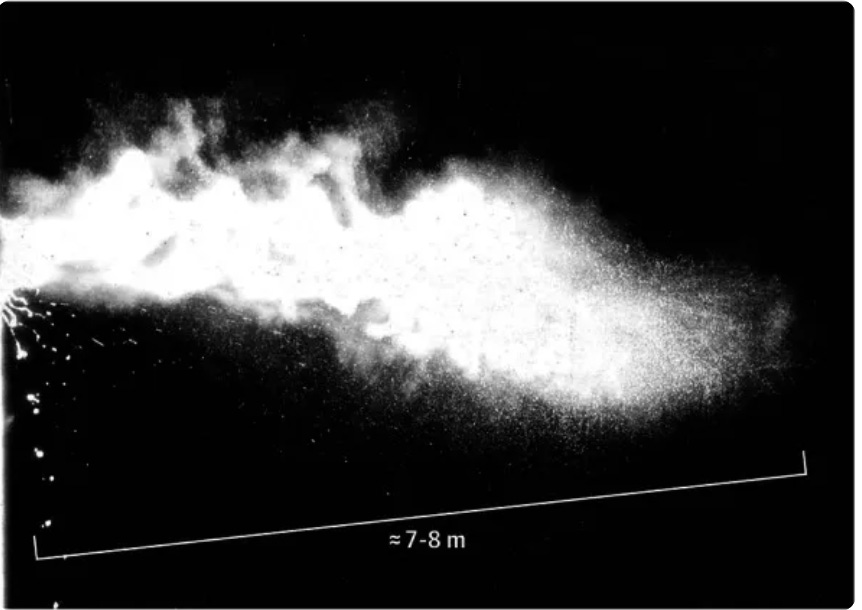
Anfinrud, P., Stadnytski, V., Bax, C. E., & Bax, A. (2020, April 15). Visualizing Speech-Generated Oral Fluid Droplets with Laser Light Scattering. The New England Journal of Medicine, 382, 2061-2063.
Davies, Thompson, Giri, & Kafatos. (2013, August). testing the Efficacy of Homemade Masks: Would They protect in an Influenza Pandemic? Disaster Medicine and Public Health Preparedness, 7(4), 413-418. Retrieved from Testing the Efficacy of Homemade Masks: Would they protect in an influenza Pandemic: https://www.cambridge.org/core/journals/disaster-medicine-and-public-health-preparedness/article/testing-the-efficacy-of-homemade-masks-would-they-protect-in-an-influenza-pandemic/0921A05A69A9419C862FA2F35F819D55
Konda, Prakash, Moss, Schmoldt, Grant, & Guha. (2020, April 24). Aerosol Filtration Efficiency Common Fabrics Used in Respiratory Cloth Masks. ACS Nano, 14(5), 6339-6347.
Ma, Shan, Zhang, Li, Yang, & Chen. (2020, March 31). Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. Journal of Medical Virology, 92(9), 1567-1571.
Konda, Prakash, Moss, Schmoldt, Grant, & Guha. (2020, April 24). Aerosol Filtration Efficiency Common Fabrics Used in Respiratory Cloth Masks. ACS Nano, 14(5), 6339-6347.
Lee, & Liu. (2012, March 13). On the Minimum Efficiency and the Most Penetrating Particle Size for Fibrous Filters. Journal of the Air Pollution Control Association, 30(4), 377-381.
Tang, Nicolle, Klettner, Pantelic, Wang, Suhaimi, . . . Tham. (2013, April 1). Airflow Dynamics of Human Jets: Sneezing and Breathing - Potential Sources of Infectious Aerosols. Plos One, 8(4).
Martin, & Moyer. (2000, November 30). Electrostatic Respirator Filter Media: Filter Efficiency and Most Penetrating Particle Size Effects. Applied Occupational and Environmental Hygiene, 15(8), 600-617.
Doremalen, Bushmaker, Morris, Holbrook, Gamble, Williamson, . . . Munster. (2020, March 16). Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. The New England Journal of Medicine, 382(2020), 1564-1567
Aydin, Emon, Cheng, Hong, Chamorro, & Saif. (2020, July 8). Performance of Fabrics for Home-Made Masks Against the Spread of Respiratory Infections Through Droplets: A Quantatative Mechanistic Study. MedRciv.
Davies, Thompson, Giri, & Kafatos. (2013, August). testing the Efficacy of Homemade Masks: Would They protect in an Influenza Pandemic? Disaster Medicine and Public Health Preparedness, 7(4), 413-418. Retrieved from Testing the Efficacy of Homemade Masks: Would they protect in an influenza Pandemic: https://www.cambridge.org/core/journals/disaster-medicine-and-public-health-preparedness/article/testing-the-efficacy-of-homemade-masks-would-they-protect-in-an-influenza-pandemic/0921A05A69A9419C862FA2F35F819D55
Asadi, Cappa, Barreda, Wexler, Bouvier, & Ristenpart. (2020, 24 September). Efficacy of masks and face coverings in controlling outward aerosol particle emission from expiratory activities. Scientific Reports, 10(15665).
Dancer, Tang, Marr, Miller, Morawska, & Jimenez. (2020, May 13). Putting a balance on the aerosolization debate around SARS-CoV-2. Journal of Hospital Infections, 105(3), 569-570.
Peters, Parniex, Otter, & Pittet. (2020, April 29). Putting some context to the aerosolization debate around SARS-CoV-2. Journal of Hospital Infection, 105(2), 381-382.
Gralton, & McLaws. (2010, February). Protecting healthcare workers from pandemic: N95 or surgical masks? PubMed, 38(2), 657-67.
Bartoszko, Farooqi, Alhazzani, & Loeb. (2020, July). Medical mask vs N95 respirators for preventing COVID-19 in healthcare workers: A systematic review and meta-analysis of randomized trials. Influenza and other respiratory viruses, 14(4), 365-373.
MacIntyre, & Wang. (2020, June 1). Physical distancing, face masks, and eye protection for prevention of COVID-19. The Lancet, 395(10242), 1950-1951.
Bahl, Doolan, Silva, Chughtai, Bourouiba, & MacIntyre. (2020, April 16). Airborne or Droplet Precautions for Health Workers Treating Coronavirus Disease 2019. The Journal of Infectious Diseases, 189.
Leung, n. H., Chu, D. K., Shiu, E. Y., Chan, K.-H., McDevitt, J., Hau, B. J., . . . Cowling. (2020, April 3). Respiratory virus shedding in exhaled breath and efficacy of face masks. Nature Medicine, 26, 676-680.
Johnson, Druce, Birch, & Grayson. (2009, July 15). A Quantatative Assessment of the Efficacy of Surgical Maks to Filter Influenza Virus in Patients with Acute Influenza Infection. Clinical Infectious Disease, 49(2), 275-277.
Green, Davidson, Panlilio, Jensen, Jin, Gibbs, & Scarpino. (2012, Mar 16). Effectiveness of selected surgical masks in arresting vegetative cells and endospores when worn by simulated contagious patients. PubMed, 33(5), 487-94.
Li, Pei, Chen, Song, Zhang, Yang, & Shaman. (2010, May 1). Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Pub Med, 368(6490), 489-493.
Tang, Nicolle, Pantelic, Koh, Wang, Amin, . . . Tham. (2012, April 20). Airflow Dynamics of Coughing in Healthy Human Volunteers by Shadowgraph Imaging: An Aid to Aerosol Infection Control. Plos One, 7(4).
Tang, Nicolle, Klettner, Pantelic, Wang, Suhaimi, . . . Tham. (2013, April 1). Airflow Dynamics of Human Jets: Sneezing and Breathing - Potential Sources of Infectious Aerosols. Plos One, 8(4).
Dancer, Tang, Marr, Miller, Morawska, & Jimenez. (2020, May 13). Putting a balance on the aerosolization debate around SARS-CoV-2. Journal of Hospital Infections, 105(3), 569-570.
Dancer, Tang, Marr, Miller, Morawska, & Jimenez. (2020, May 13). Putting a balance on the aerosolization debate around SARS-CoV-2. Journal of Hospital Infections, 105(3), 569-570.
Wynne, A. (2020, March 30). Revealed: Chorister super-spreader passed the virus to 45 out of 60 people at a Washington singing practice - as medics say transmission was AIRBORNE because they all had social distancing. Retrieved from Dailymail.com: https://www.dailymail.co.uk/news/article-8167369/Chorister-super-spreader-passed-virus-45-60-people-Washington-singing-practice.html
Li, Qian, Hang, Chen, Hong, Liang, . . . Kang. (2020, April 28). Evidence of probable aerosol transmission of SARS-CoV-2 in poorly ventilated restaurant. MedRxiv.
Dancer, Tang, Marr, Miller, Morawska, & Jimenez. (2020, May 13). Putting a balance on the aerosolization debate around SARS-CoV-2. Journal of Hospital Infections, 105(3), 569-570.
Syed, Sopwith, Regan, & Bellis. (2003, November). Behind the mask. Journey through an epidemic: some observations of contrasting public health responses to SARS. Journal of Epidemiological Community health., 57(11), 855-856.
Leffler, Ing, Lykins, Hogan, McKeown, & Gryzbowski. (2020, June). Association of country-wide coronavirus mortality with demographics, testing, lockdowns, and public wearing of masks (Update June 15, 2020). Retrieved from Research Gate: https://www.researchgate.net/publication/342198360_Association_of_country-wide_coronavirus_mortality_with_demographics_testing_lockdowns_and_public_wearing_of_masks_Update_June_15_2020.
Lyu, W., & Wehby, G. L. (2020, June 16). Community Use of Face Masks and COVID-19: Evidence From a Natural Experiment of State Mandates in the US. Health Affairs, 39(8).
Cheng, Wong, Chuang, Hung, Ho, & Yuen. (2020, July 01). The role of community wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. Journal of Infection, 81(1), 107-114.
Anfinrud, P., Stadnytski, V., Bax, C. E., & Bax, A. (2020, April 15). Visualizing Speech-Generated Oral Fluid Droplets with Laser Light Scattering. The New England Journal of Medicine, 382, 2061-2063.
Lai, & Christiani. (2013, Mar). Long-term respiratory health effects in textile workers. Pub Med, 19(2), 152-157.
Shi, Hang, Mehta, Zhang, Dai, Su, . . . Christiani. (2010). Long-term Effects of Work Cessation on Respiratory Health of Textile Workers. American Journal of Respiratory and Critical Care Medicine, 182.
Wang, Zhang, Sun, Dai, Hang, Eisen, . . . Christiani. (2005). A 20 year follow-up study on chronic respiratory effects of exposure to cotton dust. European Respiratory Journal, 26, 881-886.
Estlander. (1988). Allergic dermatoses and respiratory diseases from reactive dyes. Contact Dermatology, 18, 290-297.
Sadro, Duhra, & Foulds. (1989). Occupational dermititis from Synocril rRed 3b liquid (C1 basic Red 22). Contact Dermatology, 21, 316-320.
Seidenari, Mauzini, & Danese. (1989). Contact Sensitization to textile dyes: Description of 100 subjects. Contact Dermatology, 24, 253-258.
Rachootin, & Olsen. (1983). The risk of infertility and delayed conception associated with exposures in the Danish workplace. Journal of Occupational Medicine, 25, 394-402.
Singh, & Chadha. (2016, August 15). Textile industry and occupational cancer. Journal of Occupational Medicine and Toxicology, 11(39).
The National Academies of Sciences Engineering Medicine. (2006, April 27). Reusability of Facemasks During an Influenza Pandemic. Retrieved from The National Academies of Sciences Engineering Medicines.
Adjodah, Dinakar, Fraiberger, Rutherford, Glidden, & Gandhi. (2020, November 4). Decrease in Hospitalizations for COVID-19 after Mask Mandates in 1083 U.S. Counties. Biomedical Journal Yale.
Klompas, Morris, Sinclair, Pearson, & Shenoy. (2020, May 21). Universal Masking in Hospitals in the Covid-19 Era. The New England Journal of Medicine, 382(2020), 363.